Spinal Cord Stimulation
Spinal cord stimulation therapy masks pain signals before they reach the brain. A small device, similar to a pacemaker, delivers electrical pulses to the spinal cord. It helps people better manage their chronic pain and reduce their use of opioid medications. It may be an option if you suffer chronic back, leg, or arm pain and have not found relief with other therapies.
What is a spinal cord stimulator?
A mild electric current sends to your spinal cord with the surgically placed spinal cord stimulator (SCS) device (placed under your skin). Thin wires carry current from a pulse generator to the nerve fibers of the spinal cord. When turned on, the SCS stimulates the nerves in the area where you feel pain. The electrical pulses modify and mask the pain signal from reaching your brain, reducing the pain felt.
A spinal cord stimulator works by masking pain signals before they reach the brain. A stimulator device delivers electric pulses to electrodes placed over the spinal cord. Modified by the pulses, the brain does not perceive the pain signals or a tingling feeling replaces the signals.
Stimulation interferes with the signal to the brain, however, it does not eliminate the source of pain. The amount of pain relief varies for each person (some patients find the tingling sensation unpleasant. A trial stimulation takes place before the permanent implant so patients can see if spinal cord stimulation will work for them. The goal for spinal cord stimulation is a 50-70% reduction in pain. However, even a small amount of pain reduction can be significant if it helps you to perform your daily activities with less pain and reduces the amount of pain medication you take. Stimulation does not work for everyone. If unsuccessful, the implant can be removed and does not damage the spinal cord or nerves.
Some SCS devices use a low-frequency current to replace the pain sensation with a mild tingling feeling called paresthesia. Other SCS devices use high-frequency or burst pulses to mask the pain with no tingling feeling. Most devices have a paresthesia-free setting option.
Stimulation does not eliminate the source of pain. It simply changes the way the brain perceives it. As a result, the amount of pain relief varies for each person. The goal for SCS is a 50 to 70% reduction in pain. However, even a small amount of pain reduction can be significant if it helps you perform daily activities and reduces the amount of pain medication you take. SCS does not improve muscle strength.
SCS device systems can vary in type, however, all have three main parts:
• A pulse generator with a battery that creates the electrical pulses.
• A lead wire with a number of electrodes (8-32) that delivers electrical pulses to the spinal cord.
• A hand-held remote control that turns the device on and off and adjusts the settings.
Systems with a non-rechargeable battery need to be surgically replaced every 2 to 5 years, depending on the frequency of use. Rechargeable battery systems may last 8 to 10 years or longer, but you must remember to charge the system daily.
The pulse generator has programmable settings. Some SCS devices can sense a change in body position (sitting vs. lying down) and adapt the stimulation level to your activity. Other systems have leads that can be independently programmed to cover multiple pain areas. Some SCS devices send a sub-perception pulse with no tingling. Your doctor will select the best type of system for you.
Who is a good candidate for a spinal cord stimulator?
An evaluation of your physical condition, medication regime, and pain history will determine whether your goals of pain management
are appropriate for SCS. A neurosurgeon, physiatrist, or pain specialist will review all previous treatments and surgeries. Because
chronic pain also has emotional effects, a psychologist will assess your condition to maximize the probability of a successful outcome.
Patients selected for SCS usually have had chronic debilitating pain for more than 3 months in the lower back, leg (sciatica), or arm.
They also typically have had one or more spinal surgeries.
You may be a candidate for SCS if:
• Conservative therapies have failed.
• You would not benefit from additional surgery.
• The pain is caused by a correctable problem and should be fixed.
• You do not want further surgery because of the risks or long recovery. Sometimes SCS may be chosen over a large, complex
spine surgery.
• You do not have untreated depression or drug addiction; these should be treated prior to having an SCS.
• You have no medical conditions that would keep you from undergoing implantation.
• You have had a successful SCS trial.
SCS works better in the earlier stages of a chronic condition before a cycle of pain-suffering-disability-pain begins.
An SCS can help lessen chronic pain caused by:
• Chronic leg (sciatica) or arm pain: ongoing, persistent pain caused by arthritis, spinal stenosis, or by nerve damage.
• Failed back surgery syndrome: failure of one or more surgeries to relieve persistent arm or leg pain, but not a technical failure
of the original procedure.
• Complex regional pain syndrome: a progressive disease in which patients feel constant, chronic burning pain, typically in the
foot or hand.
• Arachnoiditis: painful inflammation and scarring of the protective lining of the spinal nerves.
• Other: stump pain, angina, peripheral vascular disease, multiple sclerosis, or spinal cord injury.
Who performs the spinal cord stimulator procedure?
Neurosurgeons and doctors who specialize in pain management (an anesthesiologist or physiatrist) implant spinal cord stimulators.
How is the spinal cord stimulator surgical decision made?
Determining whether a spinal cord stimulator will be a good option for you is a two-step process. First, you must undergo a temporary
trial to see if the device decreases your level of pain.
Stage 1. Trial “test drive”
Trial stimulation is a “test drive” to determine if an SCS will work for the type, location, and severity of your pain. It is performed at an
outpatient center.
If you take blood thinners, you are required to stop the medication 3 to 7 days prior to the trial.
A local anesthetic is given to numb the area in the lower back. Using X-ray fluoroscopy, a hollow needle is inserted through the skin into
the epidural space between the bone and spinal cord. The trial lead is inserted and positioned over specific nerves. The wires are
attached to an external generator worn on a belt (Fig. 2).
You will be sent home with instructions on how to use the trial stimulator and care for your incision site. Keep a written log of the
stimulation settings during different activities and the level of pain relief. After 4 to 7 days, you will return to the doctor’s office to discuss permanently implanting the stimulator or removing the trial leads.
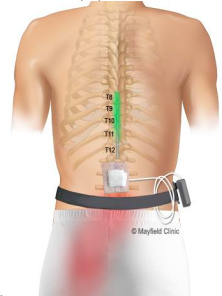 Figure 2. During a trial SCS, temporary leads are placed in the spinal canal and a stimulator is worn on a belt. For several days you will test the device to see if it relieves your pain during various activities.
Figure 2. During a trial SCS, temporary leads are placed in the spinal canal and a stimulator is worn on a belt. For several days you will test the device to see if it relieves your pain during various activities.
Stage 2. Surgical implant
After a successful trial where you feel greater than 50% improvement in pain, surgery can be scheduled to implant the SCS device in your body.
What happens before spinal cord stimulator surgery?
You may be scheduled for presurgical tests (e.g., blood test, electrocardiogram, chest X-ray) several days before surgery. In the doctor’s office, you will sign consent and other forms so that the surgeon knows your medical history (allergies, medicines/vitamins, bleeding
history, anesthesia reactions, previous surgeries). You need to Inform your healthcare provider about all the medications (over-the-counter,
prescription, herbal supplements) that you are taking.
Stop taking all non-steroidal anti-inflammatory medicines (Naprosyn, Advil, Motrin, Nuprin, Aleve, etc.) and blood thinners (Coumadin,
Plavix, etc.) 1 to 2 weeks before surgery as directed by the doctor. In addition, stop smoking, chewing tobacco, and drinking alcohol 1
the week before and 2 weeks after surgery, because these activities can cause bleeding problems. No food or drink is permitted past
midnight the night before surgery.
Morning of surgery
• Shower using antibacterial soap. Dress in freshly washed, loose-fitting clothing.
• Wear flat-heeled shoes with closed backs.
• If you have instructions to take regular medication the morning of surgery, do so with small sips of water.
• Remove make-up, hairpins, contacts, body piercings, nail polish, etc.
• Leave all valuables and jewelry at home (including wedding bands).
• Bring a list of medications (prescriptions, over-the-counter, and herbal supplements) with dosages and the times of day usually taken.
• Bring a list of allergies to medication or foods.
Arrive at the hospital 2 hours before your scheduled surgery time (1 hour before at the outpatient surgery center) to complete the
necessary paperwork and pre-procedure work-ups. An anesthesiologist will talk with you and explain the effects of anesthesia and its risks. An intravenous (IV) line will be placed in your arm.
What happens during spinal cord stimulator surgery?
The surgery generally takes 1 to 2 hours.
Step 1: prepare the patient
You will lie on your stomach on the table and be given light anesthesia. Next, preparation of the areas of your back and buttock takes place. The leads and generator will be placed here.
Step 2: Place the leads
Insertion of the electrode leads with the aid of fluoroscopy (a type of X-ray). The doctor makes a small skin incision in the middle of your back
(Fig. 3), exposing the bony vertebra.
 Figure 3. The leads require a skin incision made in the middle of your back and the generator requires another incision made in your buttock.
Figure 3. The leads require a skin incision made in the middle of your back and the generator requires another incision made in your buttock.
Removal of a portion of the bony arch (laminotomy), allows room to place the leads. The leads are positioned in the epidural space above the spinal cord and secured with sutures (Fig. 4). The leads do not directly touch your spinal cord.
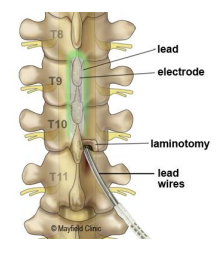 Figure 4a.
Figure 4a. 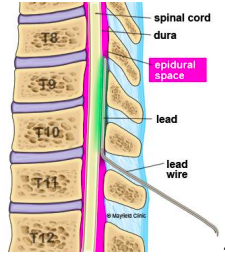 Figure 4b.
Figure 4b.
Figure 4A. A laminotomy cut in the bone makes room to insert the leads into the spinal canal.
Figure 4B. The leads positioned in the epidural space above the spinal cord deliver electrical current to the nerves.
Step 3: test stimulation (optional)
Depending on the SCS device being implanted, you may be awakened to help the doctor test how well the stimulation covers your pain
areas. However, modern SCS device leads can be positioned based on anatomy or electric monitoring of the nerves. Settings from the
trial will be used to program the pulse generator at the end of the surgery, so your feedback is important to ensure the best pain relief.
In some cases, if the leads implanted during the trial are positioned perfectly, there is no need to reposition or insert new leads.
Step 4. tunnel the wire
After placement of the lead electrodes, the doctor passes the wire under the skin from the spine to the buttock, where the generator will be
implanted.
Step 5. place the pulse generator
The surgeon makes a small skin incision below the waistline and creates a pocket for the generator beneath the skin (Fig. 5). The lead wire attaches to the pulse generator. The surgeon correctly positions the generator within the skin pocket.
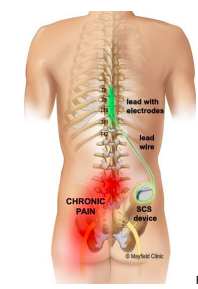 Figure 5. The surgeon creates the SCS generator pocket below the waist, under the skin of the buttock.
Figure 5. The surgeon creates the SCS generator pocket below the waist, under the skin of the buttock.
Step 6. close the incisions
Sutures and skin glue close the incision. Application of a dressing occurs.
What happens after spinal cord stimulator surgery?
You will wake up in the recovery area. Your blood pressure, heart rate, and respiration will be monitored, and your pain will be
addressed. Most patients are discharged home the same day or the following morning. The pulse generator will be programmed before
you leave. You will be given written instructions to follow when you go home.
Discharge instructions for the first 2 weeks
Restrictions
• Do not bend, lift, twist your back or reach overhead for the next 6 weeks. This is to prevent the leads from moving out of place
until it heals.
• Don’t lift anything heavier than 5 pounds.
• No strenuous activity including yard work, housework, and sex.
• Don’t drive until your follow-up appointment.
• Don’t drink alcohol. It thins the blood and increases the risk of bleeding. Also, don’t mix alcohol with pain medicines.
Incision Care
• Wash your hands thoroughly before and after cleaning your incision to prevent infection.
• You may shower the day after surgery.
• Gently wash the incision covered in Derma bond skin glue with soap and water every day. Don’t rub or pick at the glue. Pat dry.
• Don’t soak the incision in a bath, pool, or tub.
• Don’t apply lotions or ointments on the incision.
• If there is drainage, cover the incision with a dry gauze dressing. If drainage soaks through two or more dressings in a day, call the office. • Some clear, pinkish drainage from the incision is normal. Watch for increased volume of drainage or spreading redness. The infected incision may have colored drainage and begin to separate.
Medications
• Take pain medication as directed by your surgeon. Reduce the amount and frequency as your pain subsides. If you don’t need the pain medicine, don’t take it.
• Narcotics can cause constipation. Drink lots of water and eat high-fiber foods. Stool softeners and laxatives can help move the bowels. Colace, Senokot, Dulcolax, and Miralax are over-the-counter options.
Managing pain
• Ice your incision 3-4 times per day for 15-20 minutes to reduce pain and swelling.
• Don’t sit or lie in one position longer than an hour unless you are sleeping. Stiffness leads to more pain.
• Spinal headaches may be caused by leakage of cerebrospinal fluid around the lead site. The leak often heals on it’s own. Lie flat and drink plenty of caffeinated non-carbonated fluids (tea, coffee).
Activity
• Get up and walk 5-10 minutes every 3-4 hours. Gradually increase your walking time, as you are able.
When to Call Your Doctor
• Fever over 101.5° F (unrelieved by Tylenol)
• Unrelieved nausea or vomiting.
• Severe unrelieved pain.
• Signs of incision infection.
• Rash or itching at the incision (allergy to Dermabond skin glue).
• Swelling and tenderness in the calf of one leg (a sign of a blood clot).
• New onset of tingling, numbness, or weakness in the arms or legs.
• Dizziness, confusion, nausea, or excessive sleepiness.
• Fluid may accumulate under the skin around the leads or the device, creating a visible swelling (seroma). Call the doctor if this occurs.
• Sudden severe back pain, sudden onset of leg weakness and spasm, loss of bladder and/or bowel function – this is an emergency – go to a hospital and call your surgeon.
Recovery
Approximately 10 days after surgery you will come to the office to have the incision checked. Bring your device remote and product box to your follow-up appointment with the surgeon. The programming of the pulse generator can be adjusted at this time if needed. It is important to work with your doctor to adjust your medications and refine the programming of the stimulator.
Your pain specialist and device representative will work with you to fine-tune adjustments to the SCS.
Physical Therapy
Physical therapists diagnose and treat patients with medical problems or injuries that limit their ability to take part in their daily lives. Patients will usually see a physical therapist after a referral by their primary physician. Physical therapists work with patients who have experienced an injury or disease that has affected their movement and range of motion.
Your provider may recommend starting physical therapy after your procedure. After the initial follow-up appointment, your provider will determine if it is necessary or not.
What are the results of spinal cord stimulator surgery?
The results of SCS depend on careful patient selection, successful trial stimulation, proper surgical technique, and patient education. Stimulation does not cure the condition that is causing pain. Rather, it helps patients manage their pain. SCS is considered successful if the pain is reduced by at least half. Published studies of spinal cord stimulation show good to excellent long-term relief in 50 to 80% of patients suffering from chronic pain [1-6]. One study reports that 24% of patients improved sufficiently to return to gainful employment or housework with stimulation alone or with the addition of occasional oral pain medication [7]. SCS therapy is reversible. If a patient decides at any time to discontinue, the electrode wires and generator can all be removed.
What are the risks of spinal cord stimulator surgery?
No surgery is without risks. General complications of any surgery include bleeding, infection, blood clots, and reactions to anesthesia.
Specific complications related to SCS may include:
• Undesirable changes in stimulation (can possibly be related to cellular changes in tissue around electrodes, changes in
electrode position, loose electrical connections, and/or lead failure)
• Epidural hemorrhage, hematoma, infection, spinal cord compression, and/or paralysis (can be caused by placing a lead in the
epidural space during a surgical procedure)
• Battery failure and/or battery leakage
• Cerebrospinal fluid leak
• Persistent pain at the electrode or stimulator site
• A pocket of clear fluid (seroma) at the implant site. Seromas usually disappear by themselves but may require a drain.
• Lead migration, which can result in changes in stimulation and reduction in pain relief
• Allergic response to implant materials
• Generator migration and/or local skin erosion
• Paralysis, weakness, clumsiness, numbness, or pain below the level of implantation
Conditions for which you might need additional surgery include movement of the lead, breakage of the lead or extension wire, or (in rare cases) mechanical failure of the device. Reasons for removal of the device include infection and failure to relieve pain. Sometimes scar tissue develops around the electrode and can make the stimulation less effective.
What is living with a spinal cord stimulator like?
Once the SCS has been programmed, you are sent home with instructions for regulating the stimulation by controlling the strength and the duration of each stimulation period. Your doctor may alter the pulse width, amplitude, and frequencies on follow-up visits if necessary.
The pulse generator has programmable settings:
1. Frequency (rate): number of times stimulation is delivered per second. Too few pulses result in no sensation. Too many results in a washboard or bumpy effect.
2. Pulse width: the area the stimulation will cover.
3. Pulse amplitude: determines the threshold of perception of pain.
The handheld programmer lets you turn the stimulator on and off, select programs, and adjust the strength of the stimulation. Most people are given multiple programs to achieve the best possible pain relief at any point throughout the day or during specific activities.
You can use your spinal cord stimulator around the clock if necessary.
Some people feel differences in stimulation intensity depending on their position (e.g., sitting versus standing). This is caused by variations in the spread of electricity as you change positions and is normal.
Just like a cardiac pacemaker, your stimulator cannot be damaged by devices such as cellular phones, pagers, microwaves, security doors, and anti-theft sensors. Be sure to carry your Implanted Device Identification card when flying, since the device is detected at airport security gates. Department store and airport security gates or theft detectors may cause an increase or decrease in stimulation
when you pass through the gate. This sensation is temporary and should not harm your system. However, as a precaution, you should turn off your system before passing through the security gates.
The various SCS systems have different restrictions to their use with MRI, ultrasound, defibrillator, electrocautery, diathermy, and cardiac pacemakers. Be sure to know the limitations of your specific SCS device. Also, chiropractic manipulation may cause the lead to move. Consult your surgeon first.
If you believe you or a loved one may be a candidate for spinal cord stimulator surgery, contact us. Pain management is possible, let Nextgen Wellness Group help you begin healing.
Our mission is to help patients to return to work, improve their quality of life, reduce dependence on medication and healthcare providers, and avoid persistent injuries.
Related Links & Resources
Conditions & Services
Pain Management
Auto Injury
Workplace Injury
Personal Injury
Neck & Back Injury
Knee Pain
Joint Pain
Regenerative Medicine
Physical Therapy
Aquatic Therapy
Vestibular Rehab
Traumatic Brain Injury
We’re Always Just Around the Corner.
Our clinics are conveniently located to provide care for the DFW area.


Arlington, TX
801 Road to Six Flags West, Suite 146
Arlington, TX 76012
Click to Call Arlington Office